
Intussusception : causes, types , pathophysiology,features,dx and treatment
Intussusception is a condition in which one segment of intestine "telescopes" inside of another, causing an intestinal obstruction (blockage). Although intussusception can occur anywhere in the gastrointestinal tract, it usually occurs at the junction of the small and large intestines. The obstruction can cause swelling and inflammation that can lead to intestinal injury. The exact cause of intussusception is unknown. In most cases, it is preceded by a virus that produces swelling of the lining of the intestine, which then slips into the intestine below. In some children, it is caused by a condition that the child is born with, such as a polyp or diverticulum. The main symptom of intussusception is severe, crampy abdominal pain alternating with periods of no pain. Painful episodes may last 10 to 15 minutes or longer, followed by periods of 20 to 30 minutes of no pain, after which the pain returns. After symptoms have been present for a while, some children may become lethargic (feel very tired). Small children may draw their knees up to their chest during the episodes of pain. Other possible symptoms of intussusception include nausea, vomiting, and rectal bleeding (red jelly-like stools), sometimes mixed with mucus. These symptoms begin suddenly, usually one week after a non-specific viral illness. Although intussusception can sometimes be felt as an abdominal mass during a physical examination, ultrasonography is able to identify the mass with 100 percent accuracy, and is the first radiologic test ordered for patients who are thought to have intussusception. Two other radiologic tests--barium enema and air contrast enema--also are used to help diagnose intussusception. Once intussusception is diagnosed, the next step is to attempt reduction (to push the intestine back) using a liquid contrast enema or air contrast enema (the same tests that are used for diagnosis). This is a radiologic procedure, not a surgical procedure, and the patient does not need anesthesia. The liquid contrast enema and air contrast enema procedures have a 60 to 70 percent success rate, with a 6 to 10 percent rate of intussusception recurrence (return). They have a low risk of complications, as well. If radiologic reduction is unsuccessful, then the patient will need surgery. Surgery may also be done if there is a great deal of infection, or if the patient is too ill for the radiologic procedure. Show us your support by SUBSCRIBING,LIKING and SHARING. Connect with us on our website www.medcrine.com Follow us on twitter @medcrine Telegram at https://t.me/medcrine
🎬 More from Medcrine
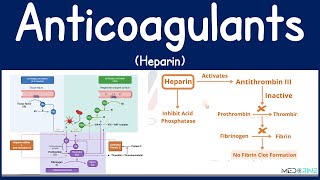
Anticoagulants: Heparin Mechanisms, Clinical Use, and Monitoring and Clinical Insights
1.2K views
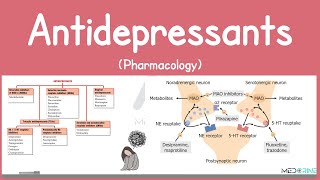
Antidepressants Pharmacology | SSRIs, SNRIs, TCAs, MAOIs, Atypical Antidepressants Simplified
1.0K views
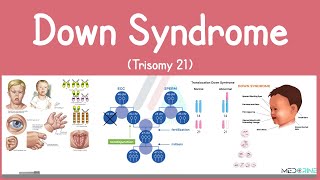
Down syndrome (Trisomy 21) - causes, symptoms, diagnosis, & pathology
376 views
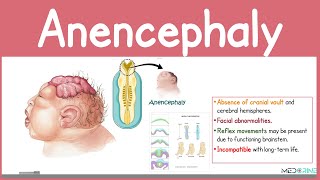
Anencephaly Explained | Neural Tube Defect | Medical and Nursing High-yield Tutorial
1.2K views
Achondroplasia | Causes, Pathophysiology, Symptoms, Diagnosis, and Management Simplified
959 views
Tension Pneumothorax: Pathophysiology, Clinical signs & Symptoms, Diagnosis and treatment Explained
580 views